
You are currently browsing the tag archive for the ‘Gail Mandel’ tag.
Housed in the nucleus of every cell in the body is 6 feet of DNA. The nucleus is so small that 10,000 of them with a combined total of 11 miles of DNA would fit on the tip of a needle. The video below explains how the unimaginable feat of coiling this amount of DNA is accomplished.
Today the journal, Cell, published research from the lab of Gail Mandel showing that the Rett protein, MeCP2, plays a role in how DNA is packaged into the nucleus. This research was funded, in part, by RSRT through the MECP2 Consortium. Using a technology called array tomography the Mandel lab found that in cells that are missing MeCP2 the DNA is more tightly compacted.
Increased compaction “hides” genes from the cellular machinery needed for protein production. So genes that are compacted are less likely to be producing protein.

Imagine DNA as a slinky with genes along the coils. In a compressed state it is difficult for these genes to be accessed by the necessary molecules that facilitate protein production.

However when the slinky is stretched out the genes become very accessible for protein production.
The scientists also found that the degree of DNA compaction was correlated to the degree of MeCP2 requirement in a given cell type. For example, cells that typically require large amounts of MeCP2 (eg. Purkinje cells) will suffer a greater change in compaction when MeCP2 is missing than cells who normally have a smaller requirement of MeCP2 (eg. astrocytes).
The video below shows normal nuclear compaction in Purkinje cells of female mice on the left and Rett mutant mice on the right.
The person responsible for this work, Mike Linhoff of the Mandel lab, describes the video, “The white shows DNA, while the green shows DNA sequences where MeCP2 binds. Red shows a particular protein modification that promotes DNA compaction. In the absence of MeCP2 this compacting modification invades the DNA sequences where MeCP2 usually binds.”
“The clinical relevance of the work is to point towards cures that will take into account neuronal-specific effects of MeCP2 loss. Once such strategy, which RSRT is already pursuing, is to reactivate the silent MECP2 on the inactive X. Other strategies might include identifying factors that can titrate gene therapy levels of MeCP2 in different neuronal types, or identifying a druggable common downstream consequence that occurs in all neuronal types,” shares Gail Mandel.
by Monica Coenraads
As always at RSRT, our funded projects are aimed at developing effective treatments and a cure for Rett Syndrome. But one of the key roadblocks to achieving this has been a lack of knowledge about the MeCP2 protein and how it functions. In 2011 RSRT decided to conduct an experiment of our own. Take three world-class laboratories and give them the necessary financial resources ($5.5 million awarded to date) and infrastructure to tackle a question that no one yet has been able to answer: what does the MeCP2 protein do?
Almost four years later the labs of Gail Mandel (Oregon Health and Science University), Michael Greenberg (Harvard University), and Adrian Bird (University of Edinburgh) are getting closer to that answer and have made the following discoveries along the way— discoveries that could prove to be invaluable to how we will ultimately change the lives of girls and women afflicted with Rett:
- It was known that MeCP2 binds to DNA in brain cells, but the Consortium showed that MeCP2 has a binding partner, called NCOR, that is known to silence genes. Importantly, the Consortium showed that mutations that disrupt the ability of MeCP2 to bind to NCOR are associated with Rett in people, thus lending support for the essential nature of this interaction.
- MeCP2 is modulated by phosphorylation for normal nervous system function.
- The Consortium has shown that gene therapy can reverse symptoms in symptomatic female Rett mice. This work is being actively followed up by a dedicated “Gene Therapy Consortium” also funded by RSRT.
- As yet unpublished work is shedding light on the crucial question of which genes in the brain are controlled by MeCP2. It may be possible to target these genes via specific drugs.

The MECP2 Consortium meets in Boston twice a year and holds conference calls in between the meetings. The meetings at first included only Professors Mandel, Bird and Greenberg but have grown over time to include many of the lab members. The middle and right pictures are from the last meeting in October 2014.
Recently I posed a few questions to the three investigators about the important work they are tackling.
Why is uncovering the function of MeCP2 important?
 Despite much effort, there is little consensus among scientists regarding what MeCP2 actually does in the brain. Needless to say it helps greatly when fixing something to know exactly what has gone wrong, so this is an issue that badly needs addressing. Fortunately the research tools for getting at the problem have gotten much better over the past few years and we are now in a good position to nail this problem down.
Despite much effort, there is little consensus among scientists regarding what MeCP2 actually does in the brain. Needless to say it helps greatly when fixing something to know exactly what has gone wrong, so this is an issue that badly needs addressing. Fortunately the research tools for getting at the problem have gotten much better over the past few years and we are now in a good position to nail this problem down.
 It’s important to know why the loss of MeCP2 gives rise to Rett as well as helping to determine a minimally active form that might be better suited to gene replacement approaches.
It’s important to know why the loss of MeCP2 gives rise to Rett as well as helping to determine a minimally active form that might be better suited to gene replacement approaches.
Is it necessary to know the function of MeCP2 to discover treatments?
 It is hard for me to imagine a treatment for Rett that isn’t based on an understanding of MeCP2 function. Based on what we already know about MeCP2 it is clear that it’s function in neurons is quite complex and difficult to understand. That together with the complexity of the brain makes me think it is unlikely that a therapy that isn’t based on a deep understanding of MeCP2 function is likely to work. Nevertheless, I wouldn’t rule it out.
It is hard for me to imagine a treatment for Rett that isn’t based on an understanding of MeCP2 function. Based on what we already know about MeCP2 it is clear that it’s function in neurons is quite complex and difficult to understand. That together with the complexity of the brain makes me think it is unlikely that a therapy that isn’t based on a deep understanding of MeCP2 function is likely to work. Nevertheless, I wouldn’t rule it out.
If we could correct the genetic changes that cause MeCP2 to dysfunction in Rett so that the defective gene is replaced by a healthy one, then we would not need to know how MeCP2 works. This ideal scenario is becoming less of a fantasy, but is still some ways from being a reality. Knowing precisely what pathways MeCP2 regulates offers the prospect of treating downstream effects of the mutation as an alternative to correcting the gene. It is too early to say at the moment which approach is more likely to bear fruit so it is important to try both.
How has being part of the Consortium impacted your lab’s research?
I think investigators in other disciplines would love to have what we have built together. The Consortium is a wonderful stimulus for new ways of thinking critically about how to study and/or cure Rett. Two heads, or in this case three heads, are always better than one, particularly because we have different expertise and backgrounds. And we can build on each other’s discoveries much more quickly.
The Consortium is a new way of working that has benefited our lab’s work greatly. Being able to thrash out ideas and explore different ways of looking at Rett with top class scientists from different backgrounds has sharpened up everybody’s research. All the partners have fully committed to the Consortium idea and as a result no one feels inhibited about robustly questioning the others. This kind of free and frank exchange keeps us on our toes and always makes research better. As well as ideas and data, we share materials and equipment, which speeds up our work and reduces costs.
How would you describe the experience of working collaboratively? Has anything surprised you?
Science is usually built on a competitive model where PIs compete for funding and try to make and publish discoveries ahead of their peers. Sharing data and plans for experiments with people who were once competitors is a different way of working – but one that is also liberating. It requires trust and a recognition by everyone that a higher goal is at stake. This Consortium really works. Hopefully we are poised to advance our knowledge of MeCP2 in ways that will make a difference therapeutically.
It has been very rewarding. Nothing really has surprised me because I knew Adrian Bird and Mike Greenberg pretty well beforehand and I had ultimate confidence in the high quality of their science and their collegiality.
Participating in the Consortium and working collaboratively with the Mandel and Bird labs has been a wonderful experience. The rigor and pace of scientific progress is much greater with the three labs working together than would be possible if each lab were working alone. Monica has been essential to keeping the Consortium on target and helping make sure the scientists in the Consortium continue to work together effectively over time.
The lab members from the three labs have thoughts of their own about the MECP2 Consortium.
| Consortium Research Projects | Reflections on Meeting | |
| Harrison Gabel (Greenberg lab)  |
Benyam Kinde, Caitlin Gilbert, William Renthal and myself have been studying how MECP2 functions when it is bound to DNA in neurons and how it might control the levels of many proteins important for the function of neurons in the brain. This exciting work may provide an answer to the long-standing question of exactly what goes wrong in individual neurons in the Rett Syndrome brain when MeCP2 is lost. I described recent results from experiments using cultured mouse neurons that lack MeCP2 to test whether drugs can correct the defects in these neurons. Promising results from these experiments suggest that a drug can at least partially correct these defects. We are now beginning to explore if this drug can improve symptoms in mice with Rett Syndrome by delivering the drug to the brain of these mice. | In general it is truly unprecedented to have three powerhouse labs that work on the mechanism of MeCP2 get together for a meeting and share their most recent data. The reality is that under any other circumstances we would be competing (hopefully in a congenial way!) and largely keeping secrets from one another until the data were published. This Consortium breaks down these walls and as a result the science moves much faster. I commend Adrian, Gail, and Mike for being willing to share so much, all of the lab members for trusting in the other Consortium members to treat them fairly, and most of all RSRT for creating such a unique and effective Consortium. Thanks! |
| Benyam Kinde (Greenberg lab)  |
At the meeting I spoke about experiments that provide insight into the mechanism of MeCP2-mediated gene regulation. Through a series of biochemical, genetic and genomic experiments, I described how DNA methylation, specifically occurring in the CA dinucleotide sequence context in neurons, serves as a critical site for MeCP2 binding and regulation of gene expression in the developing brain. | The Consortium has provided a unique opportunity to share novel findings, which ultimately has led to invaluable discussions that provide critical insight into the design and interpretation of experiments. In this way, the Consortium has allowed all three laboratories to develop projects at an exceedingly rapid pace. |
| Matt Lyst (Greenberg lab)  |
Last year we published evidence for a model where the primary function of MeCP2 is to recruit the NCoR/SMRT co-repressor complex to chromatin. At the last Consortium meeting I presented work aimed at further testing this hypothesis, and also investigating which components of this complex are most relevant to Rett Syndrome. |
Sharing current data between labs means we all receive input from people in the field but outside of our own labs at a much earlier stage than would normally happen. |
| Sabine Lagger (Bird lab)  |
MeCP2 is classically described as a methyl DNA binding protein exerting its function by exclusively binding to methylated CpG dinucleotides. It became obvious in recent years that MeCP2 can not only bind to methyl CpG dinucleotides but has been suggested to bind to other forms of modified DNA in in vitro experiments broadening its DNA binding sites. My work aims at establishing in vivo models to analyze MeCP2 binding patterns in brain cells. I therefore sort neuronal and glial cells from mouse brain and subject them to DNA methylation analysis to the single base pair resolution level. I can then overlay these maps with MECP2 binding profiles and identify the true in vivo MeCP2 targets. This analysis will help us to understand how MeCP2 is acting on chromatin and what the necessary signal for its binding are. | I was invited to the RSRT Consortium meetings in Boston twice and both times I could not wait to get back to the lab and start working again. The possibility to present and discuss my work with like- minded and enthusiastic experts on MeCP2 is extremely beneficial and made me look at scientific problems from different angles. Meeting Rett Syndrome patients’ parents was very interesting for me and made me realize even more how important it is to keep working on understanding this devastating disease and to ultimately find a cure. |
| John Connelly (Bird lab)  |
The MeCP2 protein acts by interacting with DNA at many locations inside cells. It is not clear however exactly what DNA sequences MeCP2 binds to on chromosomes. My work aims to identify what these sequences are. My hope is that understanding how the protein works in greater detail will aid the design of an effective therapeutic strategy. |
I was really pleased to be able to attend the recent MeCP2 Consortium meeting in Boston as it was really nice to meet and talk to the parents of children with Rett syndrome and discuss my work with them and the other scientists present. When in Boston I found that other members of the Consortium had, reassuringly, reached similar conclusions and this gave me the impetus to continue my particular avenue of investigation. |
| Hume Akahori-Stroud (Greenberg lab)  |
I talked about a series of experiments on understanding the role of DNA methylation patterning in the brain. DNA methylation is a chemical modification of DNA that is abundant in neurons, and regulates MeCP2 function. Understanding the molecular mechanisms of DNA methylation in regulating MeCP2 is important to understand how MeCP2 works. | It was great getting to know what other laboratories were up to, and I think the meeting has increased my understanding on MeCP2 a step further. |
| John Sinnamon (Mandel lab)  |
Many of the mutations in MeCP2, which cause Rett Syndrome are single nucleotide changes known as point mutations. Our goal is to harness the catalytic activity of an enzyme already found in cells to target and correct these mutations in MeCP2 RNA. We have been able to edit MeCP2 RNA in vitro and are working towards testing our strategy in a mouse containing a point mutation, which has been identified in several Rett patients. | Attending the RSRT Consortium meetings is a wonderful experience. There is a collaborative atmosphere you do not see at large scientific meetings and everyone is focused on understanding the biology of MeCP2 so that we can understand Rett Syndrome. For me personally, it is very powerful to meet parents of girls with Rett and to talk to them about my research. It provides a reminder of what I am working towards and I think gives the families an opportunity to talk one on one with the scientists they support. |
| Ruth Shah (Bird lab)  |
My project involves modeling Rett – causing mutations in human neurons. Model systems are a great way to elucidate the molecular mechanisms behind diseases and to understand how a protein works in a cellular context. I really hope these human neurons will help us to understand the details involved in Rett, they may even provide a useful tool for testing gene therapy ideas in! | Being part of the Consortium meeting gave me the opportunity to meet neuroscientists and gain advice and ideas from them on how to improve my project and my research. The flexibility to present my project in detail to an experienced audience without fear of my project being torn apart is a great thing. It provides the freedom for open chat and encouragement and an exchange of thoughts and ideas in a positive manner, rather than having a competitive undertone to the day. This is the environment that is needed in scientific research to encourage advances in knowledge. It allows for collaboration in a productive manner, for example as a result of the Consortium, I now have a list of genes whose expression I should look into from one of the other attending labs. If it weren’t for the Consortium I doubt information like this would be shared among labs in such an open manner. |
| Jackie Guy (Bird lab)  |
Using information we have about the MECP2 mutations found in girls with Rett we have been able to identify two important regions of the protein: the region that binds to methylated DNA (MBD) and a small region which binds to a repressor complex, NCoR/SMRT. I am producing a number of different mutations in mouse embryonic stem cells in order to investigate why they cause Rett Syndrome. This may lead to a better understanding of the function and/or structure of MeCP2. | I enjoyed hearing about the work of the other two groups in the Consortium. Each group has its own particular view of what MeCP2 is doing and I found it refreshing to think about things from a slightly different angle. |
| Rebekah Tillotson (Bird lab)  |
Missense mutations that cause Rett are almost all located in either the region of MeCP2 protein that binds to methylated DNA or the region that interacts with the NCoR/SMRT repressor complex. This suggests that the function of MeCP2 is to form a ‘bridge’ between chromatin and the repressor proteins, and loss of this bridge results in brain dysfunction in Rett. I am testing this hypothesis by manipulating the MeCP2 gene in mice, and then carrying out behavioral tests to determine whether they exhibit the symptoms observed in the mouse models of Rett. | The RSRT Consortium was a great opportunity for me to meet other scientists in the field, to learn about and discuss their work, and to get valuable input on my own project. The informality and openness of the discussion made it a thoroughly rewarding and stimulating experience. |
| Kyla Brown (Bird lab)  |
Rett Syndrome severity varies partly because of the nature of the MECP2 mutation. My project focuses on making animal models of “milder” mutations to see if there are specific functions of MeCP2 that these mutations affect. | The Consortium provides a unique opportunity to communicate findings within a group of expert researchers as well as to forge collaborations. I enjoyed being able to appreciate others’ perspectives on the same clinical and biological problem and seeing how this can result in advances in the MeCP2 field. |
| Martha Koerner (Bird lab)  |
I am working on MeCP2 duplication syndrome. I am trying to understand what happens if you do have too much MeCP2 and what we can do to counteract the symptoms caused by excess MeCP2. | The Consortium meeting in October was the first one I’ve attended. I’ve found it incredibly helpful to be able to talk to other scientists who work on the same gene, to learn about novel findings of others that will impact my research and also to get input from experts into the work I’m doing. |
| Susan Su (Greenberg lab)  |
I am interested in examining the ultrastructural changes underlying the altered cellular morphology and synaptic connections of a mouse model of Rett Syndrome. | I enjoy our lively, intellectual discussions at the Consortium meetings where we all share a common goal of gaining a deeper understanding of MeCP2. The Consortium meetings are wonderful opportunities to reflect on preliminary data and to share helpful reagents and insights for our experiments. |
| Jim Selfridge (Bird lab)  |
My work in the Bird Lab focuses on the production and analyses of genetically modified animal models of Rett. These models have proved invaluable to Rett research over the years and the novel models continue to increase our understanding of MeCP2 function and the underlying molecular basis of Rett. I am also committed to using these Rett models to investigate potential therapeutic strategies. | Although I never actually presented any of my research in person at the last meeting I was still able to benefit hugely by attending. The Consortium meetings and in particular the relaxed, open and friendly format provide a great focus for Rett researchers. It gives us a perfect opportunity to have our work critically assessed by experts in the field, even in the early stages of a project. This often affords us extra insight that we might not get from the sometimes insular environment of our own individual groups. I look forward to being part of many more meetings! |
| Will Renthal (Greenberg lab)  |
Rett is characterized by profound synaptic dysfunction. I am studying the role MeCP2 plays in coordinating the gene programs responsible for normal synaptic responses to neuronal activity. Specifically, our laboratory has found that neuronal activity drives the rapid phosphorylation of MeCP2 at serine 86, so my current efforts are aimed at identifying the functional significance of this event. | I think the Consortium was a fantastic opportunity to share ideas with people from a variety of backgrounds to accelerate Rett research. We were having technical difficulties with some of our experiments and the collective wisdom of the Consortium has been crucial for overcoming them. |
| Justyna Cholewa-Waclaw (Bird lab)  |
The aim of my project is to define primary transcriptional consequences of MeCP2 depletion. In order to do that I use an in vitro system based on immortalized human neural precursors which can be differentiated into dopaminergic neurons. I generated cells with reduced amount of MeCP2, entirely depleted MeCP2 and increased levels of MeCP2. Gene expression changes in these cells with different levels of MeCP2 will be studied additionally in the context of gene body methylation and hydroxymethylation to provide the molecular basis of MeCP2 function. | I think the Consortium meetings are great. The informal nature is very beneficial. I had brilliant opportunity to discuss my work with people working on the same problem. I could also ask questions more openly and know what other people are doing. |
by Monica Coenraads
I am delighted to give you a brief update on the MECP2 Gene Therapy Consortium, the collaboration of four elite labs that RSRT launched earlier this year. As you know, the Consortium is charged with developing gene therapy techniques that could treat or significantly reverse the symptoms of Rett. Our goal is to get to clinical trials. The project is grounded in work done last year by Consortium members Gail Mandel and Brian Kaspar that showed for the first time reversal of Rett symptoms in mice using gene therapy techniques that have the potential to be used in humans. The reversal of symptoms in mice was quite remarkable, but there are many challenges to translating that to a reversal in girls and women with Rett. The Consortium is attacking these challenges head on.
Earlier this month members of the Consortium met in the boardroom of a JFK Airport hotel in New York (we did not want to waste any of our meeting time traveling to and from a hotel in Manhattan). In addition to Gail Mandel, other members of the Consortium are Stuart Cobb (University of Glasgow), Steven Gray (University of North Carolina at Chapel Hill), and Brian Kaspar (Nationwide Children’s Hospital). The Consortium has a timeline of 3 years and a budget of $1.5 million. RSRT hosts in-person Consortium meetings twice a year as well as regularly scheduled conference calls.

From left moving clockwise:
Sarah Sinnet (Gray lab), Steve Gray, Brian Kaspar, Stuart Cobb, Saurabh Garg (Mandel lab), Kamal Gadalla (Cobb lab).
Guest participant Ruth Shah (Bird lab) joined the meeting by Skype as did Gail Mandel and Mark Bailey.

The advantages gained by labs working collaboratively are clear: speed (four labs contributing to the work that has to be done), real time sharing of information means more brainpower and broader perspectives for problem solving. This is an obvious example of more heads are better than one.
Three facts make Rett Syndrome an attractive disease for gene therapy: it is monogenic; it is remarkably reversible in animal models; delivering MECP2 does not require understanding its function.
There are several hurdles to overcome. There is a requirement for MECP2 in every part of the brain so the gene will need to be broadly delivered. Also, the MECP2 Duplication Syndrome suggests that too much MECP2 is bad. It is difficult in gene therapy to regulate how many copies of a gene enter a cell and how much protein is made so the issue of MECP2 dosage must be carefully explored. We know that having too much MECP2 from conception and through early development causes serious symptoms. But does the same hold true if extra MECP2 is delivered later in life? Also, is it possible that females tolerate greater amounts of this protein than males? These questions must be answered before a clinical trial can be proposed.
 Consortium members are also working on the following key issues:
Consortium members are also working on the following key issues:
1) Vector optimization – The vector is the Trojan horse that delivers the gene into a cell. There are many types of vectors in use and many more under development. For Rett we need a vector that can get into the brain and spread efficiently throughout the organ. The delivery route will affect the vector of choice. For example, if you deliver intravenously (via the blood stream) there is concern that a large amount of vector will end up in the liver potentially causing toxicity. To get around this problem a vector that de-targets the liver would be very useful. If dosage of MECP2 turns out to be problematic vectors that can be turned off will be required.
2) MEPC2 optimization – There are limits to the amount of DNA that can be packaged into a vector. The entire MECP2 gene does not fit. Scientists therefore have to select the parts of the gene they think are the most important. In essence they need to design a “mini-MECP2 gene’. Similar “mini-gene” work is also underway in the lab of Adrian Bird and will be shared with the Consortium.
3) Delivery route optimization – Gene therapy can be delivered via the blood stream, intrathecally into the spinal cord (like an epidural), or directly to the brain. Each route has its own advantages and disadvantages.
4) Optimizing how much gene therapy to deliver – the scientists are delivering low, medium and high dosages in an attempt to see how much is needed to get a therapeutic effect without generating toxic side effects.
We thank our precious donors who make this critical research possible!
In Their Own Words

It is very stimulating to be part of such a focused group of experts on gene therapy approaches towards Rett. The previous studies that we performed in collaboration with the Kaspar group were promising in showing that expression of a good copy of MeCP2, delivered systemically with AAV9, ameliorated Rett-like symptoms in female mice and prolonged survival significantly in affected males. Most surprisingly, but importantly, although we did not achieve a large amount of expression of the good MeCP2 in brains of the treated mice, we still saw behavioral benefits. We are now trying to improve the expression level of delivered MeCP2 by redesigning the vector, according to ideas and experimental results presented at the Consortium meetings. The openness of the investigators propels our studies and makes for a productive venture that would not be possible by any one individual laboratory. Additionally, it saves time because we can move on from doing obvious experiments that were done already in another laboratory. Finally, for those crucial experiments that had positive results, we have the ability to reproduce them in a different laboratory to insure that the results are solid.
– Gail Mandel
 The Kaspar Laboratory is extremely excited about the potential to deliver gene therapies to the CNS. We are encouraged with our delivery studies to target cells efficiently in the brain, where one requires the proper expression of MECP2. Furthermore, our clinical trial in Spinal Muscular Atrophy has to date demonstrated the safety of this gene therapeutic in children which is excellent news for development of gene therapeutics in diseases, such as Rett. As a laboratory, we have bolstered our Rett efforts and are making great progress in testing the safety and developing the pre-clinical data necessary for developing a treatment. Our approach is building off the success of our collaboration with Dr. Gail Mandel. We are thankful for her continued support on our steep learning curve of Rett. This Consortium allows us to learn from each other’s studies. It’s a great group of scientists and I’m privileged to be a part of it. I see the progress we are collectively making and the commitment to the development of a therapy for Rett patients. The path is starting to look much clearer to get there.
The Kaspar Laboratory is extremely excited about the potential to deliver gene therapies to the CNS. We are encouraged with our delivery studies to target cells efficiently in the brain, where one requires the proper expression of MECP2. Furthermore, our clinical trial in Spinal Muscular Atrophy has to date demonstrated the safety of this gene therapeutic in children which is excellent news for development of gene therapeutics in diseases, such as Rett. As a laboratory, we have bolstered our Rett efforts and are making great progress in testing the safety and developing the pre-clinical data necessary for developing a treatment. Our approach is building off the success of our collaboration with Dr. Gail Mandel. We are thankful for her continued support on our steep learning curve of Rett. This Consortium allows us to learn from each other’s studies. It’s a great group of scientists and I’m privileged to be a part of it. I see the progress we are collectively making and the commitment to the development of a therapy for Rett patients. The path is starting to look much clearer to get there.
– Brian Kaspar
 The Cobb lab shares Brian’s excitement about the consortium’s efforts and the potential for gene therapy to counteract the root cause of Rett Syndrome. The project is progressing on multiple fronts from vector design/optimization to assessing best delivery methods and testing for efficacy and safety. Whilst the concept of gene therapy is a very simple one, the route to developing a safe and effective therapy is not at all straightforward. A key element of the consortium is that it enables us to share ideas and to discuss and act on emerging results from the four labs in real time. This will inevitably lead to more rapid progress in addressing the various challenges. As well as coordinating efforts, the consortium also enables us to cross validate key experiments to ensure findings are robust and reproducible across laboratories. After our Consortium meeting Kamal and I traveled to visit Steve Gray’s lab at UNC Chapel Hill. It was an extremely valuable few days as we were able to not only observe but also practice various delivery route methods. We also were able to compare and standardize how we score neurological features seen in the mice. Spending time together also provided an opportunity to further discuss vector development. Our trip to the US for both the Consortium meeting and visit to UNC was very productive.
The Cobb lab shares Brian’s excitement about the consortium’s efforts and the potential for gene therapy to counteract the root cause of Rett Syndrome. The project is progressing on multiple fronts from vector design/optimization to assessing best delivery methods and testing for efficacy and safety. Whilst the concept of gene therapy is a very simple one, the route to developing a safe and effective therapy is not at all straightforward. A key element of the consortium is that it enables us to share ideas and to discuss and act on emerging results from the four labs in real time. This will inevitably lead to more rapid progress in addressing the various challenges. As well as coordinating efforts, the consortium also enables us to cross validate key experiments to ensure findings are robust and reproducible across laboratories. After our Consortium meeting Kamal and I traveled to visit Steve Gray’s lab at UNC Chapel Hill. It was an extremely valuable few days as we were able to not only observe but also practice various delivery route methods. We also were able to compare and standardize how we score neurological features seen in the mice. Spending time together also provided an opportunity to further discuss vector development. Our trip to the US for both the Consortium meeting and visit to UNC was very productive.
– Stuart Cobb
 Our efforts to treat Rett syndrome are built on 7 years of experience with the Rett community along with “bench to bedside” approaches that we are taking for six other inherited diseases. Our gene therapy clinical trial for Giant Axonal Neuropathy laid an important foundation for a similar approach to be taken with Rett syndrome. Gene therapy for Rett is an enormous challenge, but the last few years have garnered a great deal of excitement based on the similar positive findings published by all 4 laboratories in this consortium in 2 seminal papers. We are excited to be part of this group, and together we can accomplish much more than my lab alone. When Dr. Cobb visited our lab recently he provided critical expertise in a short visit that saved us an enormous amount of time and effort if we had been working alone. This is a small example of the many benefits we have had from working together in a collaborative fashion.
Our efforts to treat Rett syndrome are built on 7 years of experience with the Rett community along with “bench to bedside” approaches that we are taking for six other inherited diseases. Our gene therapy clinical trial for Giant Axonal Neuropathy laid an important foundation for a similar approach to be taken with Rett syndrome. Gene therapy for Rett is an enormous challenge, but the last few years have garnered a great deal of excitement based on the similar positive findings published by all 4 laboratories in this consortium in 2 seminal papers. We are excited to be part of this group, and together we can accomplish much more than my lab alone. When Dr. Cobb visited our lab recently he provided critical expertise in a short visit that saved us an enormous amount of time and effort if we had been working alone. This is a small example of the many benefits we have had from working together in a collaborative fashion.
– Steve Gray
by Monica Coenraads
[Italian translation]
[Spanish translation]
[Press Release]
Faced with the complex problem of discovering the elusive function of the Rett protein, RSRT set out to conduct an experiment of our own. We shook the conventional practice of laboratories working in isolation and instead convened three scientists to work collaboratively: the MECP2 Consortium. We gave them the necessary financial resources and provided infrastructure including in-person meetings. The results surprised us all.

Adrian Bird

Michael Greenberg

Gail Mandel
The MECP2 Consortium was launched in 2011 with a $1 million lead gift by Tony and Kathy Schoener.
RSRT has committed an additional $3.4 million of funding to the Consortium.
We are extremely grateful to the Schoeners for their second $1 million pledge to support this effort.
The Consortium quickly reported significant advancements. The Mandel and Bird labs showed, for the first time, a dramatic reversal of symptoms in fully symptomatic Rett mice using gene therapy techniques that could be utilized in people.
The “Rett mouse” moving around received healthy Mecp2 via gene therapy. The immobile mouse did not receive treatment. The video was taken four weeks after treatment.
The Bird lab discovered that the function of the Rett protein, MeCP2, depends on its ability to recruit a novel binding partner, NCoR/SMRT to DNA. Disrupt that ability and the symptoms of Rett ensue.
The Greenberg lab built on the work of the Bird lab and discovered that adding a phosphate group to MeCP2 alters its ability to interact with NCoR/SMRT and affects the expression of downstream genes.
While the clinical implications of the gene therapy experiments are obvious some may think “so what?” when it comes to the NCoR experiments.
I suspect that in the mind of many Rett parents the best evidence of research progress is clinical trials. However, this is often not the best measure of progress.
Thomas Südhof, recent Nobel Laureate, recently commented “I strongly feel that attempts to bypass a basic understanding of disease and just to get to therapies immediately are a misguided and extremely expensive mistake. The fact is that for many of the diseases we are working on, we just don’t have an understanding at all of the pathogenesis. There really is not much to translate. So NIH and many disease foundations are pouring money into clinical trials based on the most feeble hypotheses.”
So I will argue that investing in a better understanding of MECP2 – a primary goal of this Consortium – is money well spent, as it will add to our current arsenal of strategic approaches to combat Rett.
A repurposed drug may partially treat some of the symptoms, but to achieve the kind of dramatic improvement that most parents and I ache for will likely require attacking the problem at its very root.
As Rett parents will attest to the symptoms of the disorder are numerous and devastating. Whatever MECP2 is doing, it’s acting globally on many systems in the body. A repurposed drug may partially treat some of the symptoms but to achieve the kind of dramatic improvement that most parents and I ache for will likely require attacking the problem at its very root.
There are multiple ways to achieve this end goal: gene and/or protein therapy, activating the silent MECP2, modifier genes. These are all areas in which RSRT is financially and intellectually engaged with.
In parallel, however, it is imperative to understand what MECP2 does. RSRT has therefore committed an additional $3.4 million of funding to the MECP2 Consortium. We are extremely grateful to Tony and Kathy Schoener for their second $1 million pledge to support this important project.
I recently discussed the experiences of the past few years and what lies ahead with the Consortium members.
Greenberg: Research in neuroscience is undergoing a revolution. We now have the technologies in hand to solve some of the most difficult neurobiological questions. However, progress towards answering these hard questions requires scientists working together. A single lab working alone doesn’t have the expertise or the resources to make significant progress when the scientific problem is particularly challenging.
The MECP2 Consortium is a model for something much bigger: how neuroscience overall needs to operate so that we can find therapies and cures for disease.
The MECP2 Consortium is a model for something much bigger: how neuroscience overall needs to operate so that we can find therapies and cures for disease. We are scientists in different parts of the world, working together, sharing their results long before publication, and brainstorming openly on a regular basis. The different perspectives of the three labs allow for a wonderful exchange of ideas to advance the science. I believe this is what the Consortium is all about. We have ignored the typical barriers of geography and have brought together scientists from Edinburgh, Portland, and Boston on a regular basis. The results have been stunning. There has been much more rapid progress than would have been made by the individual labs.

Consortium meeting in Boston in November of 2013.
Bird: I agree. An over arching goal of the Consortium is to understand the way the MECP2 protein works at the molecular level. We are at last starting to make real progress on this and will be testing some of the new ideas in cellular and animal models. Our ultimate aim is to use this new knowledge to provide rational approaches to therapy.
Mandel: Front and center is always our goal to find a therapy for Rett. This guides our experiments and keeps us focused. The fact that financial support comes from families who have a child with Rett and their networks makes us work harder.
Coenraads: In your opinion what are the elements that have made this consortium “work”?
Greenberg: Trust and openness, a willingness on the part of all three Principal Investigators to talk through any potential problems immediately as they come up. A willingness to check egos at the door so that we can work together for something that is more important than our individual advancement. Importantly the participants, Mandel, Bird, Greenberg and Coenraads like and trust each other.
 Bird: We all have different backgrounds and interests, but we share a commitment to understanding Rett Syndrome. We compliment each other surprisingly well.
Bird: We all have different backgrounds and interests, but we share a commitment to understanding Rett Syndrome. We compliment each other surprisingly well.
Mandel: The regular meetings and exchanges and the quality of the scientists involved have been key factors as well as the availability of sufficient funding for each of us to follow our scientific noses.
Coenraads: Fortunately science is not linear. There are technologies available now that weren’t available when the Consortium started. How does this impact your Rett research?
Greenberg: There are a lot of new technologies available – in particular Cre lines that will allow us to study the effect of MeCP2 loss in a relatively homogeneous population of neurons, CRISPR and Talen technology that will facilitate gene correction, and genomic technologies that are providing a new understanding of the role of methylation in the control of neuronal gene expression. Also, better equipment, such as microscopy will help.
Bird: The technologies for genetic modification have existed for a decade, but the advent of CRISPR has made this facile. Being able to edit genetic mistakes in patients is no longer a science fiction dream, but has become a real possibility. Exploring this option will be an important focus for the Consortium.
Coenraads: Harrison Gabel from Mike’s lab recently shared with me in an email: Our group meetings are essential to critically assessing our work. Each lab group has its own “world view,” and having that view shaken up every six months is very constructive.
So I look forward to lots more critical assessments and worldviews getting shaken as together we get to the bottom of what MeCP2 does.
* Due to the success of the MECP2 Consortium, and its positive gene therapy findings, RSRT has just announced funding for a second consortium: the MECP2 Gene Therapy Consortium. Read more about this newly formed second collaboration.
by Monica Coenraads
[Italian translation]
[Spanish translation]
[Press release]
The videos below are perhaps the most well-known in the Rett community. If you love a child with Rett then chances are you’ve watched them obsessively.
This work published in 2007 by Adrian Bird, declared to the world that Rett is reversible, but did not tell us how this could be done in people.
Fast-forward six years and the video below from the RSRT-funded labs of Gail Mandel and Adrian Bird may have given us an answer: gene therapy.
The mouse moving around was given gene therapy treatment and received healthy Mecp2 gene. The immobile mouse did not receive treatment. The video was taken four weeks after treatment.
So how do we make the giant leap from recovered mice to recovered children?
To move us towards this goal, RSRT has launched their second collaborative group – the MECP2 Gene Therapy Consortium. This new group comes after the success of RSRT’s MECP2 Consortium, established in 2011, that led to the initial encouraging gene therapy findings. With a budget of $1.5 million the members of this international gene therapy collaboration are charged with tackling the necessary experiments to get us to clinical trials as quickly as possible.
I recently caught up with the investigators to discuss this novel collaboration:
Brian Kaspar (Nationwide Children’s Hospital)
Currently working on gene therapy clinical trial for Spinal Muscular Atrophy
Stuart Cobb (University of Glasgow)
Neurophysiology lab and co-author on 2007 reversal paper with Adrian Bird
Steven Gray (UNC Chapel Hill)
Currently working on gene therapy clinical trial for Giant Axonal Neuropathy
Gail Mandel (OHSU)
Member of MECP2 Consortium and author of gene therapy paper published this summer

Brain Kaspar

Stuart Cobb

Steven Gray

Gail Mandel
Coenraads: Let’s jump right in. Why Rett? Why now?
Cobb: While there have been major advances in understanding the molecular actions of the MeCP2 protein, it is still difficult to conceive of a small ‘traditional’ drug molecule being able to mimic its function. While traditional drug approaches will likely be restricted to correcting specific aspects of what goes wrong in Rett it is conceivable that gene therapy can correct the cause of Rett at its very source and thus provide a profound recovery of function.
While traditional drug approaches will likely be restricted to correcting specific aspects of what goes wrong in Rett it is conceivable that gene therapy can correct the cause of Rett at its very source and thus provide a profound recovery of function. – Stuart Cobb
Mandel: It has been known for some time now that when MeCP2 is expressed genetically in cells throughout an MeCP2-deficient mouse, major Rett symptoms are reversible in mice. Two of the big outstanding questions then are: 1) Will this be true for humans and 2) Can we add MeCP2 back to patients and also achieve reversal? The first question is currently still an open question, although upcoming experiments using human neurons and astrocytes derived from iPSCs and xenografts (transplanting human cells into mice) may provide some important clues. The second question is challenging because currently there are no reliable ways to introduce MeCP2 throughout the brain, although recent studies in mice, funded through RSRT consortiums, suggest that AAV9-mediated transduction (delivery via a virus) might have potential. Therefore, two advancing technologies, iPSCs and AAV9 viruses, are converging to compel us to jump right in now.
Kaspar: A major advantage in Rett is that the genetic target is defined for us: MeCP2. Another advantage is that it’s not neurodegenerative – neurons don’t die. And importantly, we know that restoring the proper level of MeCP2, even later in life, at least in a mouse, results in dramatic improvements.
Why now? Because the gene therapy field now has an arsenal of powerful new tools. We have at our disposal a tool kit that can express genes for long periods of time and that can target many cell types efficiently throughout the entire nervous system. Our challenge will be to utilize our toolkit to hit the precise cells at the right expression levels. I’m certain we can accomplish this goal.
Gray: That said, the devil is in the details. We have to get MeCP2 broadly distributed throughout the whole brain, which is something that has been done in animals but not yet in humans. Just as important, we have to be very careful to get the level of MeCP2 correct – too little may not work well enough and too much could cause a different spectrum of disease.
Coenraads: What have we learned thus far regarding gene therapy for Rett?
We’ve learned that a single one-time administration of a gene therapeutic can have a clinically meaningful result in the workhorse rodent model of this disease, even when delivered later in life. The results have been quite promising, and now multiple laboratories have similar promising results, it’s not just an isolated manuscript happening in one laboratory. – Brian Kaspar
Kaspar: We’ve learned that a single one-time administration of a gene therapeutic can have a clinically meaningful result in the workhorse rodent model of this disease, even when delivered later in life. The results have been quite promising, and now multiple laboratories have similar promising results, it’s not just an isolated manuscript happening in one laboratory. Using similar approaches, multiple groups have encouraging results. That’s good for science and that’s good for Rett patients.

Steve Gray (far right) and Stuart Cobb (second from the right) at an RSRT science meeting in late 2012.
Cobb: The studies have also shown that the level of MeCP2 protein produced by the gene therapy is not producing any obvious defects in its own right and it therefore seems possible to deliver protein within limits that are tolerable to cells.
We have also learned that it is not necessary to ‘hit’ all cells with the virus, this is never going to be achievable in practice anyway. Fortunately, a substantial therapeutic impact may be achieved by delivering the gene to a subset of cells. Of course the absolute number of cells, the types of cells and location in the brain is likely to be very significant. These are important issues that will be investigated by the MECP2 Gene Therapy Consortium.
Gray: Finally, the studies tell us that we have to be very careful how we target the MeCP2 gene, to make sure too much isn’t delivered to a particular organ, such as the liver.
Coenraads: Have you ever worked in collaboration with multiple labs? What do you think are the advantages? Could there be disadvantages?
Mandel: I have been fortunate enough to be part of a productive collaboration funded by RSRT to work on how MeCP2 functions normally, and in mutants, and to do, with Kaspar’s group and Adrian Bird, the initial pilot proof of principle for gene therapy for Rett, using AAV9 vectors.
Gray: Most of my work is done in collaboration with other labs, and I’m very comfortable doing research that way. I have a small and fairly specialized lab. We aren’t experts at everything, and it is much more efficient to collaborate with someone that has expertise than try to develop it on your own. This speeds things up and raises the quality of the work. The keys to making it work are that everyone has to be fully committed, and there has to be a level of trust across the members of the consortium. Trust that you can share data openly, and trust that the work is being carried out to the highest standards. If one investigator isn’t doing their part or does sloppy science then things can fall apart.

Stuart Cobb (right) with David Katz.
Cobb: I have enjoyed a number of successful bilateral collaborations in the past but the formation of the four-lab Consortium is going to be a new venture for me. Clearly there will be big advantages in terms of pooling complementary expertise to make swift progress. However, there will also be challenges, one being the necessity to maintain very good communication within the Consortium to coordinate our efforts and work together efficiently.
Kaspar: My laboratory is engaged in a number of collaborations and they are a major reason we have been successful. Our international collaborations have given us access to patient samples as well as opened the door to new ideas and interactions that just couldn’t be accomplished sitting in isolation. Collaborations bring everyone’s experience and expertise to the table and allow the participants to rapidly answer difficult questions. We don’t always have to reach consensus but the right team will be open to sharing ideas and comfortable with hearing criticism as well as be aligned on goals and focused on the patients.
Coenraads: What are the strengths your lab brings to the table?
-

Steve Gray in his lab at UNC Chapel Hill
Gray: We are part of one of the best gene therapy centers in the world, with a vector core facility that makes hundreds of research preps and several clinical preps each year. My lab in particular has, as its primary goal, a mission to develop nervous system gene therapy platforms. We’ve made enormous strides using existing vectors to their full potential, and also leading the way to develop newer and better vectors. Also, our experience bringing our Giant Axonal Neuropathy project to clinical trial gave us experience on the process of moving a biological from the bench to the bedside.
Cobb: My own lab brings expertise in the neurobiology side in terms of accurately mapping out Rett syndrome-like features in mice and within the brain and being able to assess in detail the ability for gene therapy to improve aspects of the disorder.
Mandel: I am a basic science lab and I have strengths in applying state of the art molecular tools to questions related to gene therapy. My lab also has much expertise in histology of the brain.
Kaspar: We have successfully navigated two programs from bench research to human clinical trials. We have flexibility to focus on complex basic biology questions, while keeping in mind our goal to advance therapies towards human clinical trials.
Coenraads: Gene therapy has had a rocky road. How do you view the field at the moment?
Kaspar: Expectations and promises were far too high in the early days of gene therapy. I think transformative therapies go through this track of failing and then triumphing. One simply has to look at the field of organ transplantation as an example. I think gene therapy will triumph, but we still have much to learn and pay attention to. There is a great deal of excitement and hope in the field today. We have to be good custodians of this technology with laser focus on safety and design of human clinical trials.
Gray: There are a lot of good things happening in the field right now with patients seeing major improvements in their lives as a result of gene therapy. The first gene therapy product received full regulatory approval last year in Europe. Biotechnology companies are taking an interest in gene therapy. Frankly, it is a good time to be in the field.
Modern, safer, approaches to gene therapy are developing very rapidly and it is one of the most vibrant fields in the genetics and molecular medicine arena at the moment. – Stuart Cobb
Mandel: I think that there is a large and growing momentum now for gene therapy because of the huge advances in molecular biology and viral technologies.
Coenraads: I find that the gene therapy area is polarizing – people love it or hate it – have you encountered a similar response?
Cobb: Yes, I have indeed encountered such contrasting views. Even within the community of Rett clinicians, I have had views of gene therapy being ‘the obvious route to follow’ versus others expressing great skepticism. Interestingly, the view within industry has been more accepting, perhaps due to the massive shift towards biologicals (alternatives to classical small molecule drugs) that has occurred in recent years.
Kaspar: Typically those that are not fans of this technology focus on past failures. With any transformative findings there will be disbelievers. I’m reminded by a quote from Alexander von Humboldt: There are three stages of scientific discovery: first people deny it is true; then they deny it is important; finally they credit the wrong person.
Gray: I can’t blame some people for hating it. Gene therapy promised a lot early on, before the technology was very developed. Expectations should have been tempered somewhat while the science was worked out, but instead the field moved too fast and people got hurt. That said, I don’t think you should turn your back on a potentially revolutionary medical technology because of mistakes made over a decade ago when the field was in its infancy. If you take a fresh look at the things happening today, there is a lot of real and well-founded optimism.

Gail Mandel at a
recent RSRT meeting.
Mandel: As in any area of science, there are proponents and detractors. There are technical issues with gene therapy, such as scaling and side effects that need to be addressed before more people will lose some skepticism, although some skepticism is quite healthy and pushes us to be as rigorous as possible.
Coenraads: Dr. Kaspar, tell us a bit about your experience bringing the Spinal Muscular Atrophy project to clinical trial. How long did it take from mouse experiments to trial? How much money was invested from your lab?

Brian Kaspar (middle) at an RSRT workshop.
Kaspar: Our SMA program is quite exciting. We discovered the unique capacity for AAV9 to cross the blood brain barrier in 2009, in 2010 we were in progress to have the longest living SMA mouse in the world. We further tested safety and navigated the regulatory process including the NIH Recombinant Advisory Committee, the Food and Drug Administration and our institutional review board. Late in 2013 we were granted approval from the FDA and we will be injecting our first patients in a Phase 1/2 clinical trial early this year. It was a hectic 3-year process that cost $4 million and counting. We are excited and hopeful to help children with SMA type 1.
Coenraads: Dr. Gray, you are developing a gene therapy treatment for a disease called Giant Axonal Neuropathy. Can you tell us about your experience with that project? How far from clinical trials are you? How long did it take from mouse experiments to trial? How much money did it cost?
Gray: My GAN project has been life changing. This was the project that made the connection for me to patients and changed the way I think about research. Before then it was just about getting a good paper, or a grant, or doing the right things to advance my career. Now it is about making a real difference in the lives of people I’ve come to know and love. We’re on track to treat the first patient in the first half of 2014. We developed the treatment about 3 ½ years after starting the project, which included testing the treatment in the laboratory and developing an approach that should translate to humans. It’s taken another two years to start the trial. Our preclinical supporting studies were approximately $1.5 million. The FDA-required safety studies were another $0.75 million. We are budgeting another $1.5 million for the clinical trial. Most of these funds were provided by a small grass-roots foundation called Hannah’s Hope Fund.
Coenraads: I’m delighted that you have all agreed to collaborate. I look forward to our bi-monthly phone calls and in-person meetings twice a year. Parents all over the world will be waiting anxiously to hear about your progress. As you know, there is a lot at stake.

At the end of every year the Simons Foundation announces its list of most notable papers from the autism field. Among these are two RSRT-funded papers: the gene therapy paper from Gail Mandel and Adrian Bird and the statin paper from Monica Justice.
To profoundly impact a disorder with as many varied and debilitating symptoms as Rett Syndrome, it is likely that intervention must be directed toward the very root of the problem. There are several ways to do this: activate the silent back-up copy of the Rett gene; target modifier genes; explore gene therapy.
Today, we announce a study funded through the MECP2 Consortium suggesting that gene therapy may indeed provide a feasible approach to treat Rett Syndrome.
The work was led by Gail Mandel at Oregon Health and Sciences University in collaboration with Adrian Bird of the University of Edinburgh and Brian Kaspar of Nationwide Children’s Hospital.
 Gail Mandel with lab members |
 Adrian Bird and post-doc |
In the past sixty days, four key papers have been published detailing research advances supported financially and intellectually by RSRT. Three of those papers are funded through the MECP2 Consortium, a unique alliance launched by RSRT in 2011 among three leading labs: Bird, Greenberg (Harvard) and Mandel. If you are a donor to RSRT, the accelerated research these projects represent is the result of your money at work.
We wish to express our gratitude to all of our generous supporters and the parent organizations that make this progress possible. Special thanks to our funding partners, the Rett Syndrome Research Trust UK and the Rett Syndrome Research & Treatment Foundation.
Below are some resources to help you understand today’s announcement.
Press Release [Spanish Translation] [German Translation]
Video interview with Dr. Mandel & lab members

Adrian Bird (left) and Matt Lyst
University of Edinburgh

Michael Greenberg (right) and Dan Ebert
Harvard Medical School
It stands to reason that in our battle to cure Rett Syndrome it would be of great benefit to understand the function of the “Rett protein”, MeCP2. Towards this end RSRT launched the MECP2 Consortium in 2011, a unique $1.8 MM collaboration between three distinguished scientists, Adrian Bird, Michael Greenberg, Gail Mandel. On June 16th the first two publications from this collaborative effort are published in Nature Neuroscience and Nature. Together these papers provide further clarification of the elusive function of the MeCP2 protein and how mutations within it contribute to Rett.
We thank Kathy and Tony Schoener whose visionary $1 MM gift made the Consortium possible. We thank all of our donors and parent organizations worldwide who support us, in particular our funding partners Rett Syndrome Research Trust UK and the Rett Syndrome Research & Treatment Foundation.
We are providing a variety of resources to help you understand the progress being reported today.
Animation of Nature Neuroscience Paper (courtesy of Jeff Canavan)
Chinese Translation
Interview with Matt Lyst, post-doc in Bird lab
Interview with Michael Greenberg and Dan Ebert,
post-doc in Greenberg lab
RETT SYNDROME RESEARCH TRUST WEBSITE
by Kelly Rae Chi
Rett Syndrome is caused by a variety of mutations in the MeCP2 protein, but in some instances, MeCP2’s end is missing. A graduate student in Developmental Biology at the Baylor College of Medicine in Houston, Steven Baker, who is also in the medical scientist training program, was sifting through the clinical literature on boys with such mutations when he noticed that a tiny difference in how much of the protein’s tail is shortened—by just three amino acids—seemed to make the difference between decades of life (albeit with Rett-like deficits) and death in infancy.

Steven Baker
Baker asked his adviser, Huda Zoghbi, whether she thought those extra few amino acids could so dramatically change the clinical progression of Rett.

Huda Zoghbi
“I don’t know,” Zoghbi, Howard Hughes Medical Institute Investigator and director of the Jan and Dan Duncan Neurological Research Institute at Texas Children’s Hospital, recalls telling him, because other genetic factors could be contributing the dramatic difference in the progression of Rett. “The only way to know is to make mice that have the two different mutations.”
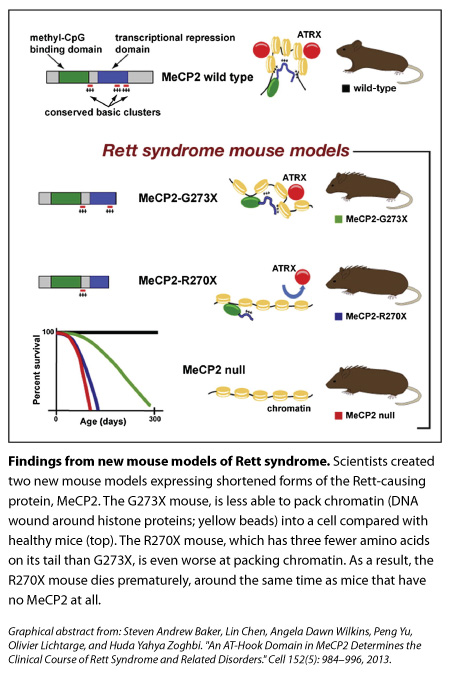
So they did. One mouse had the end of its MeCP2 cut off at the 270 mark (‘R270X’ mice) while another’s protein was shortened at the 273 mark (‘G273X’ mice). The stories of these mice were reminiscent of the boys Baker had noticed. The R270X mice died prematurely, around the same time as mice with no MeCP2. In contrast, the G273X mice, with their extra three amino acids, survived longer and showed symptoms later, although these features became more severe and the mice died before healthy mice did.
What do those amino acids do? In trying to find out, the scientists have refined their understanding of how MeCP2 works. Their results are published this week in Cell.
A first look at DNA binding:
Researchers know that MeCP2 binds throughout the genome, coating the DNA in neurons more heavily than in other cells, but what exactly it does after that is less clear. It’s thought to turn genes on or off, or alter the overall structure of DNA.
Zoghbi’s team thought that the two truncated forms of MeCP2 might bind to DNA differently — in a way that would help explain the different clinical progressions of the boys — but when they initially looked at several spots within the genome they saw that both forms bound to those spots similarly.
In fact, looking more broadly across the genome the group found that overall binding of the MeCP2 was pretty much the same, and it looked normal. (The latter wasn’t too surprising, though, because the front end of MeCP2 was already known to bind to DNA.) Both mutations also interfered with the normal ability of MeCP2 to repress genes.
Looking more closely at gene expression at various time points in brain development, however, the group found a key difference in the two mutants: at 4 weeks of age, a small group of genes was improperly expressed in the R270X mutant but not in the G273X mutant. Interestingly, most of those genes eventually became misregulated in the G273X group by 9 weeks.
The hook from the animal kingdom:
Meanwhile, the scientists asked evolutionary biologist, Olivier Lichtarge, a Professor at Baylor College of Medicine who uses computational tools to study the evolution of protein sequences, to help them compare the sequences of the protein’s tail across different species (the idea being that any regions of the protein that were highly similar across species might be important for the protein’s function). “We worked with Angela Wilkins in the Lichtarge lab and asked, ‘Is there something in this domain that’s really unique?” says Zoghbi, who is also a Professor at Baylor College of Medicine.
They found that three clusters of MeCP2’s tail were highly conserved across fish, frog, rat, mouse, and human. Shortening MeCP2 at the 273 mark removed the third of those conserved clusters, whereas cutting the tail at the 270 mark deleted the second and third clusters.
What are these clusters in MeCP2’s tail and what do they do? It turns out that they’re called AT-hooks. In 2005, a study by Adrian Bird’s group described the first of those three AT-hooks (which is the one still present in both of Zoghbi’s new models), though its function was unclear.
AT-hooks are regions of a protein that are already well known to bind DNA, however, so the team went back to the idea that the two truncated proteins might differ from one another in how they attached to the genome, even though their initial results had shown that binding was similar. Using a different assay, they found that missing the second AT-hook domain impaired the ability of the R270X to steadily interact with certain sequences in the genome.

The interaction between MeCP2 and DNA:
Our genomes are wound tightly around spool-like proteins called histones; the DNA and histones (together, called chromatin, which looks like beads on a string) are then packed in even more so that it can all fit inside cells. Using an experimental model of compaction in vitro, the team found results suggesting that R270X mice (which, remember, are missing an two AT-hooks instead of one) don’t pack up chromatin as well as 273X mice do.
The initial finding that both mutated forms of MeCP2 bind to DNA are still important though, Zoghbi says. “It tells us that the major binding to DNA happens. That’s the first step.” The researchers think that once the front end of MeCP2 sits on DNA, the AT-hook clusters on its tail come in manipulate the DNA further, likely bending or altering the structure to help it pack further into the cell.
“There were hints previously that MeCP2 might cause a change in the overall conformation of DNA. The new study is probably the most direct evidence,” says Howard Hughes Medical Institute Investigator Gail Mandel, at the Oregon Health and Science University in Portland, who was not involved with the study.
The protein partner ATRX:
When the MeCP2 sits on DNA, and likely alters the way it packs into a cell, there are other molecular partners that come and join it. One of those is the protein ATRX—whose mutations have been linked to Alpha-thalassemia mental retardation syndrome—and Adrian Bird’s lab has previously shown that its interaction with DNA is disrupted in mice missing MeCP2. Zoghbi’s team decided to look at this protein in their new mutant mice.
Compared with the healthy mice and the G273X mice, ATRX goes missing from the tightly packed DNA of neurons earlier in life for the R270X mouse, and this loss mirrors the quicker onset of Rett symptoms. “To us, that was really interesting,” Zoghbi says, “because this change is not because the neurons are sick, it’s because you don’t have MeCP2 functioning properly.”
Studying female mutant mice that are missing a copy of MeCP2, the researchers found those brain cells with no MeCP2 also had less ATRX bound to tightly packed DNA compared to controls. In female mutants with too much MeCP2, an excess of ATRX latched on to DNA. MeCP2’s absence from liver and non-brain organs didn’t affect ATRX binding in those organs, suggesting that MeCP2 has a mechanism that’s specific for the brain.
Future directions:
Taken together, these results suggest that in the brain, the AT-hook clusters on MeCP2’s tail are manipulating DNA in a way that’s crucial for the other protein partners to bind and do their jobs, Zoghbi says.
“This new paper is beginning to shed light on the complexity of this interaction between MeCP2 and ATRX,” says Mandel. In addition, “we don’t know all the other proteins that bind to MeCP2, but the guess would be that there are likely more partners affecting whether genes are on or off.”
Zoghbi’s team hopes to understand how shortening MeCP2’s tail changed chromatin structure without dramatically changing gene expression — as well as the mutation’s affect on brain activity. They also plan to do biochemical and molecular experiments to figure out where ATRX is going and what it’s doing when its distribution is altered in the brain cells of the MeCP2 mutants.
For Zoghbi, the new findings underscore the importance of going back to patients to look for clues about MeCP2’s function. In 1999, Zoghbi first showed that various mutations in MeCP2 caused Rett. “Here we are 14 years later, some of these human mutations are teaching us lessons,” she says. “The variety you get and the breadth of human features you can dissect and go back and study in the mouse are really very humbling.”
RETT SYNDROME RESEARCH TRUST WEBSITE
[SPANISH TRANSLATION]
[ITALIAN TRANSLATION]
[GERMAN TRANSLATION]
READ FULL PRESS RELEASE
On a chilly day in early spring, an unlikely group gathered in a spacious office at Harvard Medical School – the office of Michael Greenberg, Chairman of the Department of Neurobiology, one of the most respected and prolific neurobiology departments in the world. Joining Dr. Greenberg was Adrian Bird of the University of Edinburgh and Gail Mandel, a Howard Hughes Medical Investigator from Oregon Health & Sciences University. These names are well known to anyone who is at all familiar with the Rett research literature, yet none of these distinguished scientists would describe themselves as a “Rett Syndrome researcher.” The questions that have kept them busy throughout their careers revolve around basic science phenomena such as DNA methylation, gene expression and brain plasticity.
Each of these scientists has been drawn to Rett Syndrome via a different route, and their combined interests will now create a powerful synergy to explore the most basic mystery of Rett: What is the precise function of MeCP2 in the brain?
RSRT Invests Record $1.8 million in Three-Way Collaborative Experiments To Speed Path to Drug Development

Consortium: Profs. Greenberg, Bird and Mandel
Dr. Greenberg called me one day last year and said “I’m coming to you with a far-out proposition.” He confessed that elucidating the role of MeCP2 was the most challenging problem he had ever worked on (a striking remark, coming from a scientist as accomplished as Dr. Greenberg) and that the chances of success would be greatly increased if he could put his head together with outstanding researchers with complementary expertise. He asked me to explore whether there might be any mutual interest on the part of Drs. Bird and Mandel. I did so, and the response was enthusiastically positive. Synchronicity was on our side. RSRT Trustee Tony Schoener and his wife, Kathy, were interested in funding a high-impact project: the MECP2 Consortium was born.
I recently caught up with the investigators to discuss this novel and non-traditional collaboration.
Coenraads: How would the three of you define the goal of the Consortium?
Bird: The goal of the Consortium is to bring about a step-change in our understanding of the function of MeCP2 in relation to Rett Syndrome, which we believe will be vital for designing rational treatment therapies. Unlike most other autism spectrum disorders, we know exactly the root cause of this disorder, but explaining in molecular terms just why absence of functional MeCP2 brings about Rett’s particular constellation of symptoms still eludes us.
We already have useful information about what MeCP2 might do in cells – we know it is a chromosome binding protein that targets DNA methylation; we know it becomes chemically altered when nerve cells are active; and we know that other types of cells in the brain apart from nerve cells also need MeCP2 for the brain to function normally – but there is no consensus among scientists about why MeCP2 is needed for the brain to work properly.
Our joint view is that solving this tricky problem calls for cooperation between laboratories with different expertise. Gail, Mike and I have rather different slants on biology due to our training and backgrounds, but we appear to complement each other nicely. Our view is that the next few years will see advances in our understanding of both MeCP2 and the brain. The timing feels right and it will be exciting to see what happens.

Exploring the mystery of Rett

Mandel: The goal of the Consortium, from my point of view, is to put our heads together to generate new ideas, and to critically evaluate each other’s ideas and experiments, and to collaborate on experiments where the expertise is complimentary. I also view it as an opportunity to engage our young scientists in training in rigorous translational biology.
Coenraads: That is a good point Dr. Mandel. The Consortium goes well beyond the three of you. It requires the active participation of all of your lab members, who will be interacting with each other on a regular basis.

Consortium with members of the Greenberg lab
Greenberg: I propose that “speed” is a part of the equation as well. The goal of the Consortium is to gain rapid understanding of the molecular and cellular basis of Rett Syndrome through a collaborative effort.
Coenraads: During the 12 years that I’ve been working with the scientific community the concept of consortiums has been discussed from time to time. It strikes me that what differentiates a true collaboration from one that is superficial and in name only is that the desire to collaborate has to come from the scientists themselves. Collaborations cannot be imposed from above and made attractive with the bribe of money. Meaningful collaborations come from the bottom up and are nurtured by mutual respect and trust and a strong sense that the whole will be greater than the sum of its parts.
How is working with the Consortium different than how you’ve worked in the past? Has it required any kind of mental shift in your personal working style?
Mandel: Having had a long-term collaboration with my husband, who is also a scientist, I have first hand knowledge of the virtue of consortiums. My personal style has also, I think, been open to collaboration. Similarly, my lab members work very well as a team.
Bird: Science is normally a competitive activity. Discretion at least is required, if not complete secrecy, if one is to avoid the trauma of being beaten to your goal by other laboratories and scooped by their prior publication. This dog-eat-dog culture among many researchers has its advantages in that it can accelerate discovery, but is often at odds with the needs of a charity like RSRT, which may wish to have scientists putting their heads together to solve pressing, clinically relevant problems.
Our consortium intends to do the latter. We share unpublished data and resources. We speak regularly on the phone and meet several times a year to bring each other up to date on what’s new. The Consortium is still at the beginning, but already it is having an impact on the research going on in our laboratories. To be honest, I find it refreshing to be part of an endeavor that transcends our personal ambitions for a higher purpose.
Greenberg: I agree. I feel that although the Consortium research effort began just a few months ago we are already seeing a benefit. The pace of progress in understanding Rett Syndrome is already beginning to accelerate. My expectation is that through collaborative interactions with the Bird and Mandel laboratories we will be able to overcome current obstacles to understanding the molecular basis of the disorder. I think that we can expect to make key discoveries that will lead to new ideas for therapies for treating Rett Syndrome in the near future.

Coenraads: I think it’s also important to point out that the discoveries that the Consortium will likely yield will help not only Rett Syndrome but also the MECP2 Duplication Syndrome and all disorders caused by alterations in MECP2.
RSRT has committed $1.8 million to the MECP2 Consortium. The Schoeners have contributed $1 million to the endeavor. It’s an understatement to say that without them it’s unlikely we could have launched the Consortium so quickly. I thank them for their generosity, commitment and frankly, their belief in the scientific process.
To the three of you I wish you much success. I look forward to our monthly Consortium calls and in-person meetings and to keeping our readers apprised of your progress.
RETT SYNDROME RESEARCH TRUST WEBSITE
From today’s Press Release:
A paper published online today in Nature reveals that glia play a key role in preventing the progression of the most prominent Rett Syndrome symptoms displayed by mouse models of the disease: lethality, irregular breathing and apneas, hypoactivity and decreased dendritic complexity. The discovery, funded in part by the Rett Syndrome Research Trust (RSRT) was led by Gail Mandel, Ph.D., an investigator of the Howard Hughes Medical Institute at Oregon Health and Science University.
[READ FULL PRESS RELEASE]
[PRESS RELEASE – SPANISH TRANSLATION]
[PRESS RELEASE – GERMAN TRANSLATION]
 LISTEN TO PODCAST ON NEUROPOD: “MORE THAN JUST SUPPORT?”
LISTEN TO PODCAST ON NEUROPOD: “MORE THAN JUST SUPPORT?”

INTERVIEW WITH GAIL MANDEL AND DAN LIOY
Brain cells can be divided into two broad categories: neurons and glia. The three types of glial cells are the star-shaped astrocytes, the oligodendrocytes, and microglia. Historically, neurons have received most of the attention, while glia were thought to play a secondary supporting role. During the past several years it has become increasingly clear that glial cells contribute in very complex and dynamic ways to healthy brain function and are important players in Rett Syndrome.
Monica Coenraads speaks with Gail Mandel, PhD and Dan Lioy, a graduate student in her lab, to discuss their data published online today in Nature, concerning the influence of glial cells on the progression of Rett Syndrome symptoms.

Gail Mandel and Dan Lioy in the lab - Oregon Health and Sciences University
MC: It’s good to speak with you both again, and congratulations on the new Nature publication.
GM: Thanks, Monica.
MC: Let’s go back in time a little bit to give this work some context for our readers. Soon after the discovery that mutations in MECP2 cause Rett Syndrome, a researcher with a longstanding interest in chromatin, Alan Wolffe, organized a scientific meeting in Washington DC. I had just co-founded the Rett Syndrome Research Foundation, which provided financial support for this meeting. It was the first scientific meeting I attended and it stands out very prominently in my mind. And it was there, over a decade ago, that I first met you. After the meeting we stayed in touch, and I remember trying to get you involved in Rett. At first you were somewhat resistant, but eventually you really jumped in with both feet. What triggered that shift?
GM: My lab was, and is still today, working on a gene called REST, which is a repressor. We had been doing biochemical experiments and we noticed that MECP2 was one of the proteins that were in the vicinity of the REST binding sites. We didn’t know much about MECP2 so we started reading about it.
This was in 2002. Nurit Ballas was in my lab at the time, and she and I became interested in where MECP2 was in the nervous system. And we were perplexed, because it was supposed to be a ubiquitous protein, but people were thinking it wasn’t in glial cells. Basically, Nurit and I were skeptical, because we know a lot about repressors, and ubiquitous repressors in particular, and from a molecular biology standpoint, it just didn’t make a lot of sense to us that MECP2 would be excluded from glia.
So Nurit did her own experiments to search for MECP2, and she found it in purified glia, and using immunocytochemistry she showed it was in tissue—in glia in tissue. And that made us consider the possibility that MECP2 could be regulating something in glia.

Gail Mandel
MC: And that finding is a perfect example of why it’s always good in a field to reach out to new people who will bring their own experience, curiosity and fresh ways of looking at a problem. You published your first paper on the subject in early 2009 in Nature Neuroscience. Dan, please give our readers the highlights of the new paper that just came out in Nature.
DL: The key point of the paper is that in a mouse model that has no MECP2, putting MECP2 back just in astrocytes goes a long way toward correcting the Rett phenotype, especially the respiration problems. We also document that knocking out MECP2 only in astrocytes causes a phenotype, including a respiratory phenotype. But interestingly, and I’ll be the first to admit that I’m not yet clear on why this is—the phenotype isn’t complimentary to the extent of the rescue. In a simple world one would do an experiment and find that if putting MECP2 back in one cell type corrects the phenotype then removing it from that cell type should, logically cause the phenotype with equal severity. And so far, that doesn’t seem to be the case.
What I take away from our experiments is that neither MECP2-deficient neurons nor glia alone are sufficient to cause the full-blown Rett phenotype. But conversely, putting MECP2 back in just neurons or glia can go an extremely long way in correcting the phenotype. A scientifically interesting question is: Why is that?
GM: That was really the unexpected part.

Dan Lioy
DL: One possibility that we’ve discussed at length is that both cell types, neurons and glia, must be mutated to get the full phenotype. There is precedence from other diseases, like ALS, that says that neurons and glia contribute to the pathogenesis of the disease, but they do so differently. And we wonder whether or not this may actually be a general model that’s also applicable to Rett.
MC: Was this finding surprising?
GM: Yes, it was. Thankfully we did both experiments pretty much at the same time, knocking it out and putting it back. Otherwise I’m not sure we would have pursued putting it back based on the knockout. Since the knockout was not as dramatic as the null we might have concluded that glia are not very important and the disease is mostly neuronal. But, luckily, we did them both at the same time.
MC: Another example of the serendipitous nature of science. Regarding the hypothesis that neurons initiate and astrocytes play a role in the progression of the disease, do you think that’s going to become more of a common theme across diseases?
GM: That model was presented initially by Don Cleveland for ALS. I do think it is going to become a more common theme. I think it also means that we need to understand more about how neurons and glia talk to each other.
MC: Historically glia have not attracted the type of attention that neurons have, but that is changing. Gone are the days where glia were thought of simply as structural components and nursemaids to the neurons.
GM: Yes, that’s right.
MC: RSRT is funding a collaborative gene therapy project between your lab and Brian Kaspar. You are using a vector called AAV9, which, depending on when you administer it, seems to target astrocytes. If indeed replacing MECP2 in astrocytes is beneficial then this vector might be quite interesting.
GM: So this project is a big risk for my lab to take on in terms of manpower because I don’t know if it’s going to work. But I think the project is so interesting and clinically relevant. In terms of targeting the underlying genetic problem in Rett, either we turn the silent MECP2 on from the inactive X, or we have to think about how to add the gene back. That’s why I think AAV9 may hold promise, because it has good expression and it crosses the blood-brain barrier. There are a lot of labs working on gene therapy approaches so the field is competitive, but I think that is a good thing.
MC: Well, we are risk-takers—we can’t afford not to be—so we’re delighted that your lab has become so engaged with Rett and opened up new research vistas. I agree with you about the value of competition, and will follow the unfolding of the next developments in your work with great interest. There is certainly no lack of complexities to explore. We hope the Rett community will continue to benefit from your scientific curiosity and perseverance. Thanks for your time with us today, and we look forward to the next updates.

